

What is the pathway of specialty training after MRCP MRCS etc or job opportunities following these exams for an International Medical Graduate (IMG)? How will a doctor at that stage join in the specialty training pathway in the UK or even the workforce in the NHS?
These are very commonly asked questions and also very commonly we see people comparing between PLAB vs MRCP MRCS. Yes, a comparison can be made between the two exams based on the level of difficulty, cost etc but the final deciding factor should also involve knowing how your career afterwards will take shape.
The idea of ‘competency’ based specialty training for doctors
Competency
1. the ability to do something successfully or efficiently.
“This course will improve the competence of doctors”
From the beginning of pre-school to our final exam in medical school, more often than not, our ability to successfully complete a stage had been dependent on exams and assessments. For example, a student of a medical school has a curriculum (set by the authority who runs medical education in that country) and following that, a syllabus is made by the teachers involved who imparts the necessary education for that student to pass the relevant exams.
There could be provision of mini-assessments in the form of written or oral exams which finally lead to the final medical exam at the end of their program which awards them the diploma. Almost exactly the same notion applies to doctor’s specialty training in the UK.
- Training Curriculum: It is made by the faculties / Royal Colleges of that specific speciality.
- Teachers: The deaneries / Local Education Training Boards (LETBs) make sure that a trainee follows that curriculum. They appoint educational supervisors, they arrange for training days liaising with individual post-graduate medical education centres (PGMC) in all the trusts. The Royal College/Faculties also appoints ‘College Tutors’ who overview the training progression of a trainee.
- School / Institution: National Health Service (NHS) is your place of work, it is also your place to train. The deaneries have fixed number of posts within the NHS to allocate to their trainees. The rest of the posts are filled by the individual trusts with trust-grade/non-training doctors.
So, you see, a core surgical trainee, or an internal medicine trainee or a respiratory medicine trainee or WHICHEVER trainee has a curriculum to go through. That curriculum consists of different competencies.
What are these ‘core competencies’?
The competences are called core competencies because this is for ‘core level training’. You must already know what a core level training is for an uncoupled specialty. If you don’t, keep reading.
To give an example of competencies, for internal medicine training:
- Delivering effective resuscitation and managing the acutely deteriorating patient
- Communicates effectively and is able to share decision-making, while maintaining appropriate situational awareness, professional behavior and professional judgement
Now, how will a trainee prove that they can do this? By doing supervised learning events.
You can find the internal medicine training curriculum here and also find the core surgical training curriculum here.
As mentioned already these competencies are part of the curriculum made by the relevant Royal College or faculties. To get into any uncoupled specialty training bypassing their formal core level training, you HAVE to show proof that you, in some other way (non-training or non-UK work) has already achieved those competencies. This is the big target.
There is always an ‘Alternative Core Competencies Certificate’ for a core level training which need to be signed by the authorised signatories if you want to bypass going through a formal core level training.
Say for example, you have already completed MRCP and you want to join cardiology training. So you either have to go through 3 years of Internal Medicine Training (formal core level training for cardiology) OR get an ‘Alternative Core Competencies Certificate’ signed if you fulfill all the criteria mentioned there.
Find alternative core competence certificate for medical specialities here and for surgical specialities here.
A brief idea about a doctor’s training pathway in the UK
Here it is. If it is still a bit confusing about uncoupled, core level training etc. watch this video which will give you a refresher on how the whole training pathway for doctors in the UK is structured.
How to achieve an alternative certificate of core competencies?
Passing the Membership exam (if you have not already)
You can’t dream to get a alternative core competencies signed without completing the specialty related membership exam first.
Having a look the alternative core competence certificate
Just by reading the certificate, you will have an idea whether the years of your clinical work have obtained those competencies or not. You may find you haven’t done many things just because the healthcare infrastructure is different. In that case, it will not be believable if you get it signed with your non-UK work.
Getting into a non-training job in the UK
After you have obtained GMC registration, the next target would be starting in a non-training job in the UK to fill those gaps in competencies and eventually try to get into training. And you fill those gaps in your competencies by doing supervised learning events and WPBAs as mentioned in the video above.
Maintaining an e-portfolio
Like trainees, as a non-trainee doctor you can maintain your own e-portfolio as well and gather the evidences of your education and progression. But, for you, it will help you prove your alternative core competencies instead of finishing a formal training.
Audits and Quality Improvement Project
Involvement in clinical audits and quality improvement is also a major part of your core competencies.
Attend specialty relevant training courses
For surgical trainees courses like basic surgical skills, Care of the critically ill surgical patients are almost mandatory to complete.
Having clear communication with your supervising consultant
The whole thing of getting your alternative core competence certificate is done informally. That means no royal college or PGME will be asking your supervising consultant to sign this for you, YOU will have to. So having a good channel of communication with your supervising consultant is very necessary.
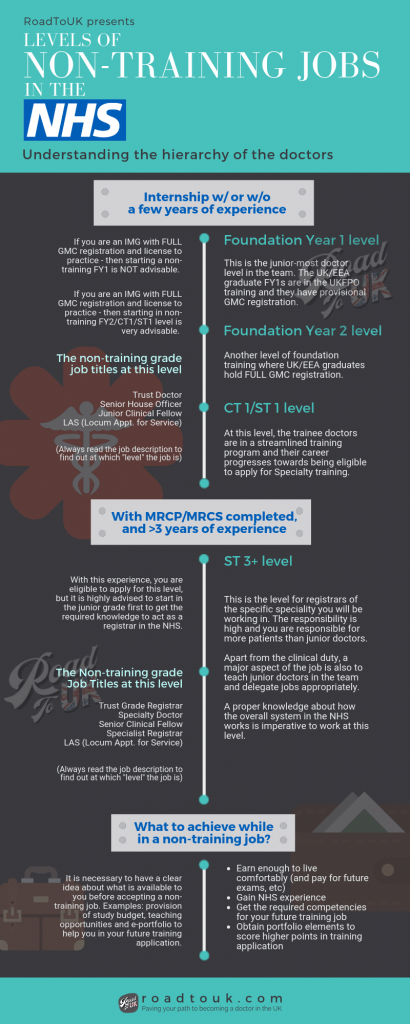
Level of jobs after completing membership exams (MRCP/MRCS)
Now as I said in the point number #3, getting into a non-training job is your entrance into the NHS. Which posts are more preferable as a job after MRCP MRCS?
Let’s first talk about the level of jobs and what they all mean. There are 3 levels of doctors in the NHS:
- Junior grade
- Middle grade
- Consultant/Senior grade
By definition, the doctors who finishes core level training and passes membership exam i.e after MRCP MRCS – they are regarded as middle grade, the specialty registrars. But for an IMG without any NHS work experience taking up that responsibility straight away can be daunting and very easy way to get dissatisfied and god forbid in trouble as well.
Our honest opinion is that, it’s always better to start as a junior grade if you don’t have any prior NHS experience, even if you’re experienced back home or have completed a post graduate qualification. You can always apply for a middle grade post after working as a junior grade for a few months.
What about other specialties membership and fellowship exams?
Unlike most medical and surgical specialties where specialty training is after MRCP MRCS, many other membership and fellowship exams are not midway between being a registrar and consultant. Some of them are in between intermediate and higher-level training during the specialty training, some of them are in between specialty and sub-specialty training.

Please check GMC Approved Post Graduate Curricula to check the pathway and exams to be taken for your desired specialty.
So if you come to the UK completing a fellowship exam like FRCA (for anaesthetics) or FRCR (for clinical radiology) or higher trainee exams like MRCOG (all parts), MRCPCH (all parts) etc you can find yourself in a tricky situation. From a qualifications point of view, you are as equivalent as a senior registrar or a consultant but from an NHS experience point of view, you have none.
For doctors like these, starting a formal training pathway can prove to be a drag or even impossible due to entry criteria restriction (overqualification in some specialties). So what would they do?
They can either look for long term SAS grade (Specialty & Associate Specialist), which is a trust grade senior doctor level post or take CESR (Certificate of Eligibility of Specialist Registration) route working in the NHS in a non-training fashion. Bottom-line, the doors will not be closed for you.
Frequently Asked Questions
Am I a consultant after completing MRCP/MRCS?
No. These exams are taken by junior residents/trainees to transition into a registrar role.
Just passing these exams does not automatically mean you get promoted or are regarded as competent in taking a higher post. You will have to have sufficient clinical experience and prove your competency to work at a higher level.
Can I join the ST3/4 level directly after MRCP/MRCS?
No. Alongside MRCP/MRCS, Full GMC Registration- you will also need alternative evidence of core competencies form signed by authorised signatories.
Will I be regarded as a consultant in my own country after MRCP/MRCS?
Unlikely, as these are not specialization exams.
Should I take PLAB or should I take MRCP?
PLAB is just a registration exam, where MRCP/MRCS are PG qualifications. Even if you take PLAB, you will have to take the membership exams to progress in your career to become a specialist. Read more here – PLAB vs MRCP: What do you need to know.